

Capabilities Framework - capabilities vs competencies
How they are different and why capabilities is a superior paradigm for public health going forward.

In my previous post, I gave some reasons why the Capabilities Framework (CF) for public health in Aotearoa New Zealand was created and how it’s better than other frameworks. The CF is:
Fit for the purpose of the day - to grow the workforce towards Pae Ora.
Comprehensive in scope covering all public health functions and workers.
Representative of and informed by the diverse and experienced National Public Health Service (NPHS) workforce - the experts about operational public health work for our communities and populations.
Another reason the CF is better than what’s gone before is the CF’s approach to professional skills as ‘capabilities’ rather than ‘competencies’. These words sound similar and are often used interchangeably, as if they mean the same thing. But there are nuanced and important differences between the concepts. It is therefore worth teasing out these differences and understanding why capabilities are a superior paradigm for public health going forward.

As we begin, if you’re a bit confused - don’t worry, you’re in good company. It took us a lot of time during the CF development to explain and demonstrate the value of capabilities. Whenever we presented to new groups we’d have to start here. It got to the point of cliche where my colleagues would often ask, as a joke, “Hey Samuel, what are capabilities again? Hahaha…” Not everyone is an HR nerd and fair enough!
We also faced scepticism from some groups about changing from competencies. There are lots of competency standards already in place and familiar across public health, and don’t we want the workforce to be competent? Why reinvent the wheel just to change definitions? (Even though public health loves stupid debates about definitions…)
I get it - I was sceptical at first too. Which is why credit deservedly goes to Ken Trass, NPHS National Learning and Development (L&D) Manager. He believed in the transformational potential of capabilities and convinced me and NPHS leadership that it was the right approach for public health instead of more competencies. We would not have reached the great outcome of the CF without his vision.1 Thanks Ken :)
Breaking down competencies
Competencies have been entrenched in human resources practice over the past 50 years as thinking and evidence about the drivers of job performance and productivity has evolved. Many sectors and organisations globally have developed competency frameworks to guide recruitment, training, and performance management including in health.
A traditional definition is usually along the lines of competencies being “the skills, knowledge, and behaviours that enable individuals to perform effectively in their roles” - which is fairly generic and sounds similar to our definition of capabilities. Indeed, there can be a spectrum between the two paradigms, and some of the modern competency frameworks actually lean more towards capabilities in my opinion. But classically they are different approaches and outlooks. Capabilities are superior and more useful for public health going forward, but in some roles and industries competencies remain appropriate.
The easiest difference to spot between competencies and capabilities is the scale of human skills being assessed. Competencies are a more micro approach, focusing on an individual’s observable and measurable attributes that contribute to the performance of specific tasks at different levels of proficiency. For example, a competency in using Microsoft Teams to set up and host virtual meetings. This task could be broken down into different levels of competence from beginner to expert depending on the user’s application of different Teams functions, the size and length of the meetings hosted, and so on.
Importantly for competencies, the performance of tasks must be measurable, as measuring enables evaluation and comparison between workers and business units. For example, two workers performing the same task at different speeds suggests variance in competency. I am a faster typist than my four-year-old son; ergo I am more competent at typing than him (take that boy!).

There is an innate appeal in being able to measure yourself and your competence. Workers often like having tangible, demonstrable evidence of their competency and progression which can be used as leverage for higher pay. Employers like it too because it sets expectations and creates consistency.
But this measurability also limits competencies as an approach. Competencies are most effective when tasks can be clearly defined and prescribed. They are therefore quite valuable in sectors where tasks are standardisable and roles can be tightly aligned to those tasks, for example in manufacturing.
But the harder it is to define and measure tasks, the less useful competencies become. When tasks are more complex, ambiguous, or context-dependent, it can become tricky to pinpoint which competencies are required, how they should be demonstrated, or how performance can be fairly assessed and compared. For example, teachers working in different countries may have the same job title and seek similar education outcomes. But the actual tasks involved may be radically different due to their students, the language and culture, the subject matter and curriculum, the equipment and resources, and so on. Attempting to do the job in exactly the same way according to the same competency definitions is likely to lead to disaster. There is therefore limited usefulness in basing comparisons on the same, micro-level competencies. The tasks need to be the same or similar enough for competencies to work well.2
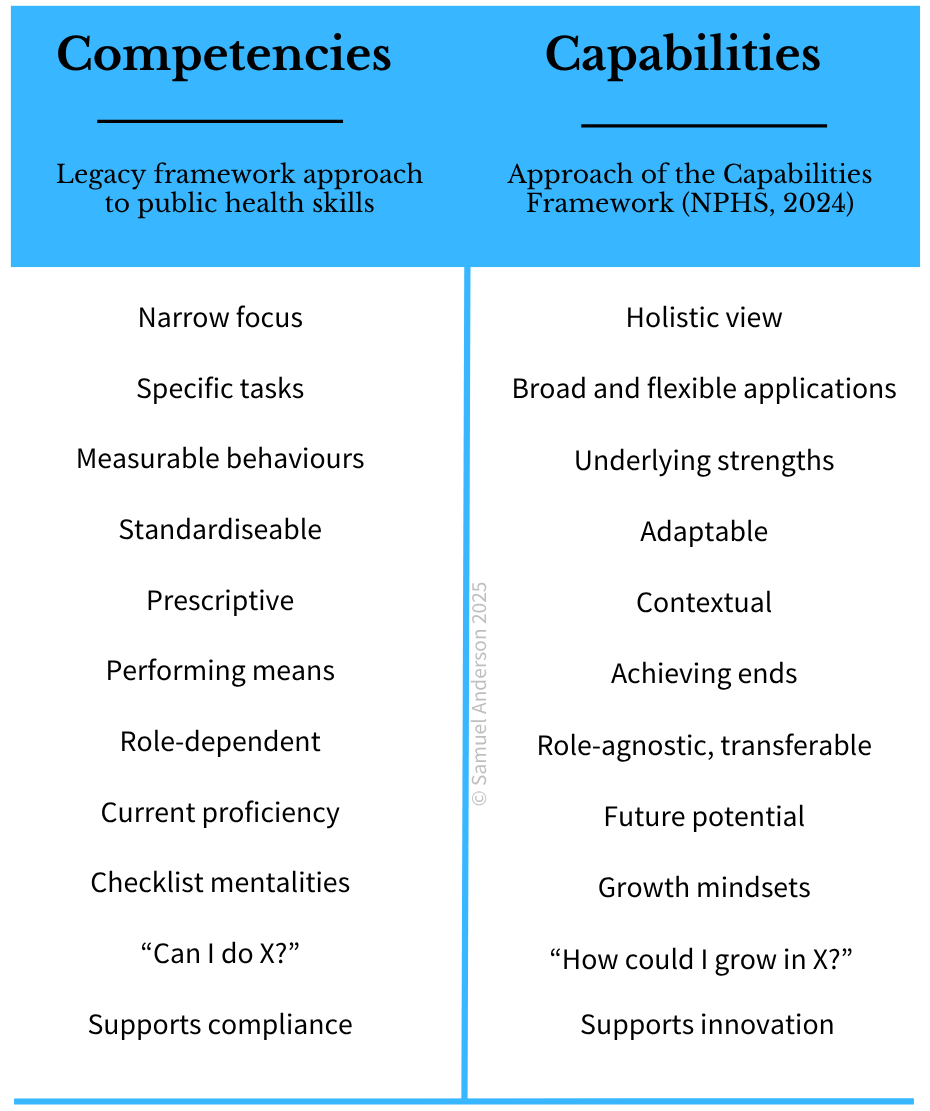
A related issue is evolving circumstances. Competencies are prescriptive and most effective when they are clearly defined to enable measuring. But when the situation changes, workers may need to do tasks differently or apply new thinking or techniques. Competencies are therefore prone to becoming outdated as their definitions cease to be relevant. Competency frameworks must therefore be continually updated to account for changes; the longer between revisions, the less useful the competencies become. Worse is when outdated competencies continue to be expected which can constrain creativity and innovation impacting on quality improvement. Transferable skills may be overlooked and emerging trends may be ignored. This can result in organisations struggling to take advantage of opportunities or overcoming new challenges.
Finally for now, competencies are limited due to their outlook and emphasis on current performance and proficiency. Competencies are typically designed to describe what someone can do now within the boundaries of existing roles and known tasks. This focus privileges the present by default. For example, the starting point for a worker figuring out how to apply competencies is usually to reflect on their current performance, asking themselves questions like:
Can I do this [specific competency] right now?
What level of proficiency am I demonstrating?
Afterwards they may seek to grow in their abilities, but if they are satisfied with their current competency, they may check that box and do nothing more. This can create blind spots going forward, where the need for adaptation may be missed resulting in performance diminishing over time.
I’m not saying don’t reflect on the present (and past).3 Continuous reflection on how you’re doing is a necessary ingredient for personal growth. But in the context of workforce and organisational performance, the purpose of examining what’s gone before is to lead us into better outcomes in the future. Achieving that potential is the true end - the goal and prize to aim for. Competencies tend to miss that by fixing us too much in the present.
Competencies and public health
So, are competencies a good fit for public health? In Aotearoa New Zealand, they have had some value historically. Currently most medical officers, nurses, and statutory officers have mandatory competencies or standards that must be maintained in order to continue in a role, make use of legislative powers, and oversee interventions and responses. These are determined by the Ministry of Health and medical professional bodies and colleges - NPHS is beginning to be involved in the review and revision of these standards. Beyond these are competency frameworks that can be adopted voluntarily by individuals to demonstrate their proficiency, for example in generic public health competencies, in Māori public health, and in health promotion.4 For these “legacy frameworks” still in effect for NPHS kaimahi (staff), the CF was designed to work alongside rather than replace them. I will discuss this dynamic further in my next post.
The legacy frameworks have been useful but for NPHS they are not adequate by themselves. Many public health disciplines and roles have had no competency or skills frameworks and have therefore relied on whatever performance indicators were written into job descriptions. While the mandatory competencies have been regularly reviewed and updated, the voluntary frameworks have been more static and outdated. And none of the frameworks are very task specific, making them less effective as tools for assessment and comparing performance. In this sense they are not even true competency frameworks, merely giving an appearance of maintaining standards by ticking a few boxes. Just to name a few issues.
Making the existing competencies more measurable and thus more competency-like would be a hard ask. Public health work is very context specific. Staff with the same role titles in one part of the country may have entirely different day-to-day responsibilities as counterparts elsewhere depending on their specific populations, environments, health determinants, and more. Some of this diversity is due to the regional public health units evolving independently during the district health board era; creating a more consistent and aligned public health service was one of the reasons for the Pae Ora reforms. But many differences will remain despite unification. Health Protection work, for example, is determined by risks from the specific local environment, climate, industries, population density, ports of entry, disease patterns, and more. Many of the same issues crop up but actions and approaches must be tailored to the situation. Adaptability is essential in public health responses. A one-size-fits-all national competency system therefore cannot afford to be overly task prescriptive.
I was fortunate to have some understanding of this prior to the CF development. In 2022, I led a project to establish individual development plans (IDPs) for all NPHS kaimahi in my home districts of Canterbury, West Coast, and South Canterbury.5 My partners and I anticipated that public health competencies could be updated as part of the health reforms (I did not foresee that I would be leading that effort), and so for the IDPs we did not reinvent the wheel, choosing to adapt the Public Health Association’s Generic Competencies for Public Health (2007) - the most recent national framework at the time.
I will say more about this framework in my next post, but adapting it to our context was a real slog. Aligning the generic competencies to each role - including assigning proficiency levels required - took months of negotiation with the various leadership teams. While the framework was helpful in providing a platform for development conversations, the 15-year-old competencies themselves were awkward and ill-fitting, with many deemed unnecessary for large numbers of kaimahi challenging whether they were actually “generic”. There were also a lot of gaps, and we had no way of objectively assessing whether kaimahi were growing in the specific competencies. In hindsight, the main outcome of the IDPs was it enabled kaimahi to re-engage in professional development post-COVID. I think that was more thanks to having a process than from the competencies themselves.
So, when the opportunity arose in 2023 for a new national framework, NPHS opted not for competencies but a new paradigm to imagine public health skills for the Pae Ora era. Doing competencies again, properly, would have required a more granular, task and job-centric approach that would not have been suitable for public health, would not meaningfully drive future performance, and would have been difficult to create and maintain given the diversity of roles across the system among other practical concerns.
But the most compelling reason for change was to shift public health’s focus from present abilities to future potential. Competencies would keep us stuck in tickbox mentalities where minimum standards being maintained are satisfactory. We need approaches that influence our attitudes towards growth and continual improvement so that collectively we can adapt and realise public health’s potential.

Capabilities - the new paradigm
Emerging from complexity theory and organisational learning research, capabilities are a more expansive and adaptive conceptualisation of professional skills than competencies. In the CF (page 12), we defined capabilities as “the broad skills, knowledge, and behaviours that NPHS needs collectively and individually to deliver on Pae Ora…”
The keyword there is “broad”. Where competencies are micro focusing on mechanistic tasks and doing things, capabilities are more macro encompassing the holistic thinking and abilities that enable people to achieve outcomes.
And when I mean outcomes, I mean the real ends that tasks are meant to serve. Take our earlier example of using Microsoft Teams to set up and host virtual meetings. Looking at Teams through a competencies lens will focus us on whether the software is used successfully. Capabilities, on the other hand, push us to consider the underlying purpose - of enabling online collaboration and communication. That’s the point of using Teams - the why, the true ends. So rather than asking “Can this person use Teams?” the capability lens invites us to ask, “Can this person facilitate meaningful collaboration in a virtual environment?” That subtle shift opens up space for creativity, adaptability, and a focus on impact rather than just technical execution. Someone might tick every competency box for operating Teams, yet still fail to engage well with others, foster trust, or achieve shared understanding - all of which are needed for effective collaboration.

Once you’re focused on the outcomes and ends, the specific means to achieve them becomes secondary. Right now, Microsoft Teams is ubiquitous across NPHS; collaborating as a national service would be much more difficult without it. But Teams is just a means of achieving that greater goal. Other software, techniques, or arrangements might achieve the same or better results. Capabilities allow for that flexibility in means and for doing things differently if the situation requires it. This enables wider skills to be drawn upon, and for the wider context to be factored in, ensuring that actions are fit for purpose. This is crucial for public health work as our earlier Health Protection example demonstrated. A capabilities approach empowers kaimahi to apply Protection knowledge as fits their local contexts and as situations evolve, ensuring better outcomes. A more overtly competencies approach, with prescribed tasks and processes, risks that actions will be less suitable and effective.6
There’s a few caveats and philosophical threads we could go down at this point.7 The means absolutely still matter, and the ends do not always justify the means. There is wisdom in having consistency of tasks, tools, and techniques, and that may be a requirement in compliance and regulatory areas. Oftentimes, doing the same thing, applying “best practice” will be best. But having consistency is not as important as getting the right outcome. I am confident that public health already understands this principle; the CF with its capability lens is merely bringing that dynamic to bear in our thinking about skills and development.
There’s a few more things to explain about capabilities and the CF before I wrap up. Flexibility is not just important in terms of skills but also in educational approaches. There are many ways to gain skills, knowledge, and behaviours; the same capability can be learned in different ways in different places. Capabilities allow for such flexibility in pedagogy. For example, learning aimed at building understandings about “the history of public health work in own local districts and communities including recent efforts” (as per the example in History of public health, CF, page 23) will look different depending on where the learning takes place, with what kaimahi and professional group, what the specific history is, and so on. The CF gives educators the strategic learning objectives for NPHS, which need to be aligned to going forward. But it is not prescriptive about learning design and gives educators space to find the right pathways to those objectives. Competencies sometimes are more restrictive in how skills must be taught.
The broad nature of capabilities also enables skills, knowledge, and behaviours to be more readily recognised as transferable or “role agnostic” - meaning they can be demonstrated and developed across a variety of roles regardless of job titles or functions. For example, the shared public health capability of “partnering with communities to understand and harness their lived experience…” (Lived experience of communities, CF, page 25) is just as relevant for a health promotion advisor engaging in community development activities as it is for an intelligence analyst interpreting trends in non-communicable disease prevalence. While their day-to-day tasks differ, both roles rely on similar underlying strengths to connect with and reflect community realities.
Recognising that capabilities are transferable and can span roles has a range of benefits including:
promoting integrated ways of working and collaboration, where people from different roles and disciplines are supported to contribute to outcomes. It encourages the question “who has the right capabilities?” rather than the narrow “whose job is this?” which can lead to silos.
enhancing workforce development, where flexible development pathways are supported enabling higher staff mobility across functions. For example, health protection staff being able to move into health promotion or PHCD (public health capacity development) work as they may already have many of the underlying strengths required.
fostering staff cohesion, where all team members can be seen as bringing valuable capabilities and make contributions to shared outcomes.
A defining strength of capabilities is their emphasis on future potential. While competencies focus on current performance and proficiency, capabilities are concerned with what people and teams can become. They recognise that learning is ongoing because what skills are needed tomorrow may be different to what we have today. This is especially important in public health where future challenges are uncertain and emerging. Continual growth, development, and improvement will support public health to navigate whatever situations we face.
What does harnessing a capabilities mindset look like then? For individuals, it is by reflecting not just on current performance but on our goals and aspirations, answering questions like:
How do I want to grow?
What kind of contributions do I want to make?
What impact could I have if I grow in this [capability]?
How can I deepen my capabilities?
What is new in this [capability area]?
How might I need to grow in future?
What would growing in my capabilities mean for me and for public health?
This kind of reflection shifts the focus from meeting standards to exploring opportunities and improvement. It empowers individuals to imagine how growth can benefit us and our teams, communities, and the public health system. Weighing up our current capabilities can be a component of this process. But to truly reach our potential we need to go further: embracing a mindset oriented towards continual learning, future possibilities, and the contributions we are yet to make.
The challenge for public health now is to embed the CF and capabilities thinking in our organisational practices to support ongoing growth across the workforce. This is a vital step in our collective journey towards Pae Ora.
How do capabilities work in the Capabilities Framework?
Finally, I want to show some of how capabilities thinking manifests in the CF. Being broad and flexible throughout was crucial. At the structural level, we chose a more abstract, core functions approach to public health rather than focusing on specific roles or professions. This encourages public health skills, knowledge, and behaviours to be seen as transferable and potentially useful for growth by anyone. We hope the CF will encourage NPHS staff to engage in learning in core functions they don’t typically work in; this will grow shared understandings and collaboration, improving our public health initiatives and organisational effectiveness.
Concerning specific capabilities, being broad and flexible meant focusing on the true and enduring ends of skills, knowledge, and behaviours. The capability statements/definitions (left side of the below example) are pitched at a higher level than competencies, giving space for individuals to demonstrate and grow in them as appropriate for their work and context.
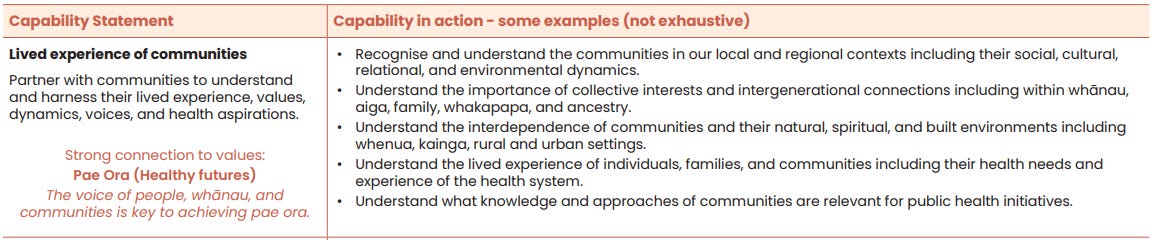
Illustrating the capability statements are the extensive examples labelled “Capability in action - some examples (not exhaustive)”. In the end, we compiled almost 1,000 of these examples across the CF, and so some might feel that they are quite exhaustive! That is what happens when you have over 200 collaborators sharing their rich experience in such a project!
There are heaps of examples, but it is still true that they are not exhaustive. There will be many more ways that these capabilities can manifest, and that will evolve over time. The absence of proficiency levels means the CF is not prescriptive about what capabilities should look like at different stages - that will evolve too. Being broad and non-prescriptive allows room for diverse expressions of strength and proficiency.
Lastly for now, is that the CF is framed as the collective growth needs of NPHS and public health. There are simply too many capabilities, and too many examples, for them to be treated like a checklist of skills to be performed. As amazing as some of our kaimahi are, that is not expected or possible. As an organisation, NPHS needs to ensure it is growing in the capabilities, but this growth will be spread across the workforce.
I like to think of the CF as a smorgasbord - a rich and varied spread where every capability has value, contributing strategically to public health. For individuals, the key questions become: which capabilities do I most need to strengthen, and in what ways do I want to grow, so I can continue to contribute to the success of public health?
I hope you too can imagine your possibilities as you engage with the CF.
Thanks for reading,
Samuel Anderson.
What’s next on Capability Matters?
I’ve got lots more planned to share about the CF. Upcoming posts include:
the legacy frameworks and how the CF relates to these;
the Te Tiriti o Waitangi, equity, and Pae Ora foundations of the CF; and
an overview of the development process.
Subscribe to Capability Matters to continue the journey with me.
If you want to get in touch, send me an email at capabilitymatters [at] proton [dot] me - inserting the obvious punctuation. Cheers.
The original demand for NPHS was actually for a curriculum for all public health workers. That was a ‘deliverable’ for NPHS in Te Pae Tata - the first operational plan for the health system to deliver on Pae Ora. But a curriculum is not a starting point and NPHS could not from scratch create a curriculum for all public health workers. You first need a framework (capabilities or competencies) or some other vision from which learning outcomes can be defined and purposed, i.e. what skills and knowledge are you trying to grow and why? This then informs education processes like the structure, design, and delivery of learning activities. That’s how you make a curriculum. So as not to do things backwards, Ken got the deliverable for a curriculum changed to a capabilities framework. Now the sector and education providers can update and create new public health curricula based on the CF, as is beginning to occur.
The same can be said about targets being evidence of delivery and performance. People like having targets, but the same critique for competencies applies as targets are often similarly prescriptive, narrow, and reductive. They also tend to be quite arbitrary. Consequently, any meaning derived from them are shallow (e.g. whether targets are being achieved and therefore whether the organisation/government is performing). Targets are only one data point and must be supported by wider evidence especially in complex sectors like health. Leaders promoting targets as the sole or primary lens to understand performance are oversimplifying by cutting out the nuance; over time problems will arise from the straitjackets they are forcing us into. (Let the reader understand).
“Context”, looking back to the past to understand the present, happens to be my top strength according to Strengthfinders.
Including international competency frameworks.
NPHS had already been formed by this time, but operationally the regional public health units were still largely working as they had before; this changed over 2023-2024. The small national L&D team was established after we had begun on IDPs, and they signalled that new national IDPs were at least a year or two away. We proceeded with our project on the conviction that it would be better for our staff to have something now (IDPs and greater access to professional development) while we waited. That was a good decision for our staff and also for me personally to have gained that experience going into the CF project.
The flexibility in means also means that capabilities are less likely to become outdated than competencies. Right now, I am a better typist than my son. But maybe keyboards will be redundant in the future?! When keyboards or Microsoft Teams become obsolete, so will any competencies and competency frameworks based on them. But the capability for communication will endure. Capabilities build in the assumption that our methods will continue to evolve.
E.g. competencies vs capabilities is the same as reductionism vs holism.